What are the risks and benefits of using vitamin C for depression and anxiety?
“In adults, emerging evidence suggests that higher daily intake of fiber-rich fruit and vegetable servings is associated with lower incidences of anxiety, greater happiness, higher life satisfaction, and greater social-emotional well-being,” says a review in the journal Nutrients. So, “persuading people to consume more fruits and vegetables may not only benefit their physical health in the long-run, but also their mental well-being in the short-run,” concluded a study in Social Science & Medicine. Fruit consumption, for example, has a protective association with leading killers like heart disease, stroke, diabetes, and cancer, as well as depression. The question is why?
Several mechanisms have been proposed. For example, one posits it’s the antioxidant and anti-inflammatory properties of produce, which scavenge the free radicals that are involved in some of the inflammation associated with depression. If that’s the case, what about simply taking vitamin C supplements? The brain has some of the highest levels of vitamin C in the body, so it’s thought that if extra vitamin C is consumed, it may have some sort of therapeutic role in brain diseases, especially given that it is not just an antioxidant, but also has other critical functions in the brain, such as helping to build neurotransmitters like dopamine. But you don’t know whether it actually helps until you put it to the test.
One study found a beneficial effect of adding vitamin C as an adjunct treatment to an antidepressant, while another study found no benefit from vitamin C supplementation.
So, there are mixed results for vitamin C and depression. Another study found no benefit when it came to depression, but those randomized to vitamin C instead of placebo pills did show a significant decrease in anxiety level. And this wasn’t only seen in that study.
The effects of oral vitamin C supplementation on anxiety in high school students were studied in a double-blind, randomized, placebo-controlled trial. The teens were given 500 mg a day of vitamin C or a placebo. That daily amount of vitamin C is about what you’d find in five oranges, four yellow kiwifruit or guavas, or one and a half yellow bell peppers. Within just two weeks, the vitamin C reduced anxiety levels compared to placebo, as well as provided a significant drop in heart rate.
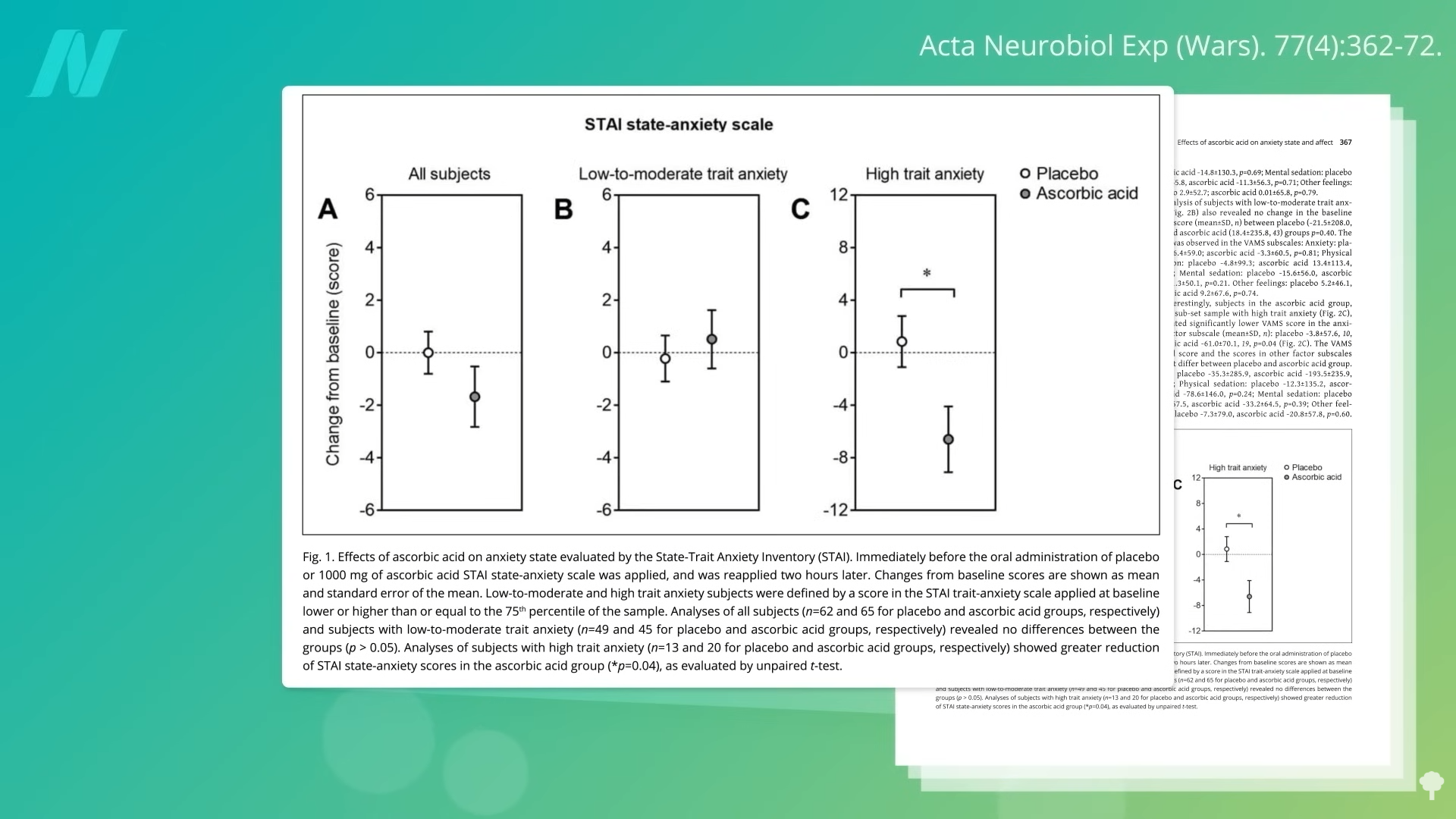
Given these data showing that vitamin C may have an anxiety-reducing effect, researchers sought to find out if a single dose could acutely affect emotional states. And indeed, within only two hours of taking some vitamin C, study participants experienced a significant drop in anxiety compared to placebo, though only among those who started out the most anxious in the first place, as you can see below and at 2:42 in my video Do Vitamin C Supplements Help With Anxiety?.
As a bonus, vitamin C supplementation may lower our blood pressure a few points, but whole fruits and vegetables can do the same thing—and may even do it better for those who need it the most, as shown below and at 2:53 in my video.
As I’ve shown previously, simply adding just two servings of fruits and vegetables a day can have psychological well-being benefits within only two weeks—and without the kidney stone risk associated with vitamin C supplements, though that appears to be only a problem in men.
Doctor’s Note
For more on vitamin C and on anxiety, check out related posts below.
Preventive care is often overlooked by people managing busy schedules, yet it remains one of the most effective ways to maintain long-term health. Preventive checkups, vaccines, and screenings help detect potential issues early, reducing the risk of serious conditions and minimizing disruptions to daily life. By staying consistent with preventive care, individuals can save both time and healthcare costs in the long run.
What Is Preventive Care and Why Is It Important?
Preventive care includes routine checkups, vaccines, and screenings designed to prevent illness or detect conditions early. Instead of reacting to symptoms, this approach focuses on maintaining health before problems arise.
For those with busy schedules, preventive care provides stability. Early detection often leads to simpler treatments, shorter recovery periods, and fewer interruptions to work and personal responsibilities. It also supports overall productivity by reducing the likelihood of unexpected health issues.
Essential Preventive Checkups You Shouldn’t Skip
Preventive checkups are the foundation of a healthy routine. Annual physical exams help assess overall health and identify potential concerns early.
Blood pressure and cholesterol checks are essential for detecting heart-related risks, which often develop without symptoms. Routine lab tests, including blood work, provide insights into blood sugar levels and organ function.
Dental and eye exams should not be neglected, as they can reveal underlying health issues beyond oral and vision concerns. For people with busy schedules, combining multiple checkups into one visit can make preventive care more manageable.
Vaccines Adults Need to Stay Protected
Vaccines are a key part of preventive healthcare, helping protect individuals and communities from infectious diseases.
The flu vaccine is recommended annually, especially for those frequently exposed to public environments. COVID-19 vaccines and boosters may still be advised depending on current health guidance.
The Tdap vaccine, which protects against tetanus, diphtheria, and pertussis, is typically required every ten years. Other vaccines, such as HPV and shingles, are recommended based on age and risk factors.
Keeping track of preventive vaccines through reminders or digital records can help individuals stay consistent despite busy schedules.
Recommended Screenings by Age and Risk
Preventive screenings help detect diseases before symptoms appear. Cancer screenings, including breast, cervical, colorectal, and prostate exams, are among the most important.
Screenings for diabetes and heart disease are also essential, particularly for those with risk factors such as family history or lifestyle habits. Mental health screenings play a growing role in preventive care, helping identify stress, anxiety, or depression early.
For older adults, bone density screenings can detect osteoporosis and reduce the risk of fractures. Following recommended preventive screenings ensures timely intervention and better health outcomes, according to Johns Hopkins Medicine.
How to Fit Preventive Care Into a Busy Schedule
Time constraints are a common barrier, but preventive care can still fit into busy schedules with proper planning.
Bundling appointments allows multiple checkups and screenings to be completed in one visit. Telehealth offers a convenient option for consultations that do not require physical exams.
Setting reminders through digital calendars or health apps helps ensure that appointments and vaccines are not missed. Choosing clinics with extended hours, including evenings or weekends, also improves accessibility.
Planning ahead and scheduling appointments early can prevent conflicts and reduce cancellations.
What Preventive Care Should Adults Get Regularly?
Adults should prioritize annual preventive checkups, routine lab tests, and recommended vaccines. Preventive screenings, including blood pressure, cholesterol, and cancer screenings, should be completed based on age and individual risk factors.
Dental and eye exams are also essential parts of a consistent preventive care routine.
How Often Should You Go for a Health Checkup?
Most adults benefit from yearly checkups, although some may require more frequent visits depending on their health status. Preventive screenings and vaccines follow different schedules, with some occurring annually and others every few years.
Which Vaccines Do Adults Need Every Year?
The flu vaccine remains the primary annual recommendation. COVID-19 boosters may also be advised periodically. Other vaccines, such as Tdap or shingles, follow longer timelines but remain important for preventive care.
What Screenings Are Recommended for Different Age Groups?
Preventive screenings vary by age and risk level. Younger adults typically focus on baseline health checks, while older adults require more comprehensive screenings for chronic conditions and cancer.
Healthcare providers tailor recommendations to ensure screenings remain relevant and effective, as per UCLA Health.
Common Mistakes Busy People Make About Preventive Care
Many people skip preventive checkups due to time constraints, assuming they are healthy without regular monitoring. Others delay vaccines and screenings, increasing the risk of undetected conditions.
Failing to track appointments and medical records can also lead to missed preventive care opportunities. Consistency is key to making preventive healthcare effective.
Quick Preventive Care Checklist
Schedule annual preventive checkups
Stay updated on vaccines
Complete recommended screenings
Track medical records and results
Set reminders for appointments
Why Preventive Care Matters for Busy Schedules
Preventive care is a practical and time-saving approach for individuals with busy schedules. Staying consistent with preventive checkups, vaccines, and screenings helps reduce health risks and avoid unexpected medical issues.
By making preventive care a priority, individuals can maintain control over their health while managing daily responsibilities more effectively.
Frequently Asked Questions
1. Can preventive care be done without health insurance?
Yes, many clinics, community health centers, and pharmacies offer low-cost preventive checkups, vaccines, and screenings.
2. Are at-home health tests reliable for preventive screenings?
Some at-home tests can be useful for initial screening, but results should still be confirmed by a healthcare provider.
3. What time of year is best to schedule preventive checkups?
Early in the year is ideal so follow-up screenings or treatments can be completed without delays.
4. Do lifestyle habits count as part of preventive care?
Yes, habits like balanced nutrition, regular exercise, and adequate sleep are essential components of preventive care alongside checkups, vaccines, and screenings.
Sometimes happiness might seem like a stretch—for us and even for our children. The stresses of daily life, getting out the door in the morning, managing a household, coordinating schedules, as well as the bigger issues, including concern about the struggles in the world, can all take a toll on us as adults. Given the increasing issues with children’s mental health, we know it’s taking a toll on our children as well.
And yet, amid difficulties, happiness is still attainable and essential to well-being and resilience. Research on adult well-being shows that there are specific steps we can take to develop and nurture happiness.
As James Baraz writes, joy is “a general feeling of aliveness and well-being that is characterized by meeting ups and downs in life with authenticity and perspective.”
Based on our work with children, we know this is true for them, as well. It can be as simple as enjoying a hug, being mesmerized by a ladybug, or giggling at the shape of a cloud. These simple pleasures can be little moments of joy for our children and for us—and they can be a part of raising happy children who are resilient, even in the middle of normal ups and downs.
Not Denying Difficulty, But Opening to Possibility
When we talk about raising happy children, we are not talking about “happiness” as the fleeting emotion that is a response to good or fun things. We are not suggesting pushing difficulties aside, but instead developing the capacity to hold them alongside our well-being. As James Baraz writes in Awakening Joy, joy is “a general feeling of aliveness and well-being that is characterized by meeting ups and downs in life with authenticity and perspective.”
We envision a happy child as one with a developing sense of ease with themselves, one who often sees and enjoys the good around them and within themselves.
Happiness is not a destination or something to be achieved, but rather what Chang Meng Tan, author of Search Inside Yourself, defines as “a deep sense of flourishing that arises from an exceptionally healthy mind.”
We envision a happy child as one with a developing sense of ease with themselves, one who often sees and enjoys the good around them and within themselves.
Research by the Center for Healthy Minds shows that well-being is a learnable skill. There are multiple evidence-based perspectives offering practical ideas for cultivating happiness.
In particular, The Resilience Project by Hugh Van Cuylenburg focuses on gratitude, empathy, and mindfulness to support resilience and happiness. The Action for Happiness Project has a similar focus and lists mindfulness, gratitude, and kindness as core skills. In Hardwiring Happiness, Rick Hanson adds to this list and stresses the importance of inclining the mind, or being on the lookout, for happiness and then taking it in.
Raising Happy Children Starts by Building Well-Being Skills Together
Here are three fun activities based on these frameworks to try with your child.
Inclining The Mind And Taking It In Practice: Glimmer Wand
Glimmers, coined by Deb Dana, are little moments of peace, safety, and happiness.
Cut out, decorate, and glue a star on top of a popsicle or other stick. You can write “catching glimmers” on the star. Share about glimmers and use the wand to “cast a spell” to notice and enjoy glimmers that day. You can also wave it overhead as people share their glimmers and how they make them feel.
The brain has a negativity bias. By pausing to seek out glimmers, we can train our brains to notice and savor delight more often.
Gratitude Practice: Gratitude Sandwich
Children can draw and cut out pictures of five things or people they are grateful for as their sandwich fillings.
Cut two pieces of paper for the sandwich bread.
Glue one piece of the “bread“ to the top and one to the bottom of a poster.
Paste the fillings between the bread (or Velcro so it’s interchangeable).
Write Gratitude Sandwich and “I am grateful for…” on the “bread.”
Leave the sandwich somewhere visible and use it as a conversation starter about gratitude.
Dr. Robert Emmons at UC Davis found that feeling gratitude can move our nervous system out of the stress response. Giving children a visual link to things that foster feelings of gratitude can help strengthen the body-brain connection and develop positive neural pathways.
Cultivating happiness can be quite simple if we focus on it, even when things are hard. Pausing to notice and take in the good, feeling gratitude, and connecting with others with empathy and kindness in the tiny moments of our day can make a genuine difference.
Connection Practice: Links of Love
Have the child think about five people who make them feel loved or happy.
String a bead for each person onto a pipe cleaner.
Twist the ends together so the beads don’t fall off. These are links of love.
Have them touch one bead at a time and remember the special person.
Take a breath in, taking in their love, and out, offering love back to them.
Encourage them to notice how they feel. The links of love can be attached to a backpack, worn around a wrist, or left in a visible location.
Especially when a child feels lonely or insecure, having a physical anchor can remind them that they are worthy and loved.
Tuning Attention Towards Happiness
Cultivating happiness can be quite simple if we focus on it, even when things are hard. Pausing to notice and take in the good, feeling gratitude, and connecting with others with empathy and kindness in the tiny moments of our day can make a genuine difference.
Fun, hands-on activities, like those above, can help both adults and children lean into happiness and create space for more joy in our lives.
Would you like more support building habits of well-being and resilience in your child? Try our new card deck, available April 21. Let’s Grow Happiness includes 50 activity cards to help kids build gratitude, self-compassion, and emotional regulation skills.
Innovel Medical, a London-based developer of clinically focused medical technologies funded by Pentland Medical, presents a perspective that airway safety outcomes may be influenced by how procurement decisions are made. This consideration becomes particularly relevant when cost factors are prioritized over purpose-built securement solutions intended to support patient safety, infection control, and tube stability.
“In operating rooms and critical care settings, airway securement is an important part of patient care that doesn’t always receive the same level of attention,” Stewart Munro, Managing Director of Innovel, states. “Clinicians recognize its role in maintaining stability during anesthesia and ventilation, though the approaches used in practice can vary.”
The implications of this variability are increasingly supported by emerging data. According to a study, unplanned extubation (UE) remains a measurable and persistent safety concern, even as structured airway safety programs demonstrate the ability to reduce its incidence. These findings, Munro argues, point to a broader opportunity for consistency in airway management practices, particularly in how devices are selected and applied.
“In many areas of medicine, practice evolves as evidence accumulates, yet airway securement has often relied on methods that were never originally designed for the task. There’s an opportunity to revisit these conventions with a more intentional lens,” he explains. Munro believes that unplanned extubation is preventable and encourages standardized securement approaches supported by reliable tools and protocols.
Within clinical settings, Munro notes that the challenges associated with non-purpose-built securement methods can present in several ways. Clinicians may encounter variability in adhesive performance, which can affect tube stability during procedures involving movement or prolonged positioning. Skin integrity can also become a consideration, particularly among pediatric and older adult patients, where repeated application and removal of general-use tape can affect the skin barrier. These factors, while often managed at the bedside, contribute to a broader picture of cumulative clinical and operational impact.
Research into ventilator-associated pneumonia (VAP) further illustrates the importance of secure airway management. A pneumonia surveillance guidance highlights the role of tube movement and micro-aspiration in bacterial contamination of the lower airway. A meta-analysis, encompassing more than 16,000 patients, found that re-intubation increased the risk of VAP by more than fivefold. Such findings, Munro stresses, reinforce the connection between airway stability and infection risk, underscoring the value of securement methods that can maintain consistency throughout the duration of care.
Munro offers an additional perspective on how these clinical realities intersect with procurement practices. “When decisions are made primarily at the unit-cost level, it can be difficult to fully account for the downstream clinical considerations that follow. Expanding the lens to include total care impact allows for a more balanced evaluation,” he remarks. This viewpoint reflects a growing conversation among healthcare leaders and procurement teams about how to align purchasing decisions with broader patient safety and system efficiency goals.
Innovel’s response to these insights is reflected in the development of LeaFix, a purpose-built airway securement device designed specifically for endotracheal applications. Engineered with a focus on both stability and skin compatibility, LeaFix incorporates a structured adhesive design that distributes pressure across anatomical anchor points, supporting consistent tube positioning. Its CE marking under the EU Medical Device Regulation (MDR) reflects adherence to stringent regulatory standards, providing an additional layer of assurance for healthcare providers seeking validated solutions and providing Innovel with real-world clinical evidence to improve its solution.
Beyond its technical features, Innovel observes that LeaFix may reflect a growing recognition of airway securement as a distinct area within clinical practice. Munro states, “In other areas of care, purpose-built devices have often been introduced over time as understanding of clinical requirements and performance expectations has developed.”
Within this context, Innovel’s broader portfolio, including complementary solutions such as packaging both eye and airway securement solutions together, is part of its ongoing focus on helping related needs across the airway management pathway. Another innovative solution from Innovel is the Vacuderm, which is a smart tourniquet with an aim to not only identify potential invisible veins, but also facilitate easier cannulation.
The conversation around airway securement is also extending into professional forums and educational initiatives. Innovel has supported a recent webinar, where clinical experts shared insights into airway-related risks and emerging best practices. Such platforms, as Munro notes, can contribute to raising awareness and fostering dialogue among clinicians, hospital leaders, and policymakers.
As healthcare systems continue to refine their approaches to patient safety, airway securement presents an opportunity for alignment between clinical insight, regulatory standards, and procurement strategy. Munro states, “Progress usually begins with recognizing areas that have remained unchanged for a long time. From there, meaningful improvements can be introduced through collaboration and thoughtful design.”
A forward path emerges through a more integrated approach to decision-making, where procurement teams consider not only immediate cost but also clinical performance, patient experience, and long-term system impact. By supporting the adoption of purpose-built, regulated solutions, healthcare organizations can move toward greater consistency in airway management, contributing to improved outcomes across diverse care settings.
The human body is constantly at work behind the scenes, performing countless automatic processes that keep a person alive and functioning. Reflexes, metabolism, hormones, inflammation, and circadian rhythms operate every day without conscious effort, yet they quietly shape energy levels, mood, and long-term health.
Understanding what these systems do, and what changes in them might mean, can offer useful insight into overall well-being.
1. Your Body’s Reflexes Are Constantly Protecting You
Reflexes are rapid, automatic responses that protect the body from immediate harm. They are controlled by the nervous system and happen without a person having to think about them, allowing the body to react faster than conscious decision-making would allow.
Simple actions like blinking when something approaches the eye, sneezing to clear irritants from the nose, or pulling a hand away from a hot surface are all examples of everyday reflexes at work.
Healthcare professionals often check reflexes during routine exams because they can reveal important information about nerve and muscle function. Slowed, exaggerated, or absent reflex responses may point to issues in the nervous system or spinal cord pathways.
While most people rarely think about their reflexes, these quick reactions are a key layer of protection built into the body’s daily routine.
2. Your Metabolism Never Truly “Stops”
Metabolism is the term for all the chemical reactions that occur in the body to convert food into energy and maintain vital functions. Even during sleep or rest, the body uses energy to support breathing, circulation, temperature control, and cell repair.
This baseline energy demand is known as the basal metabolic rate, and it represents how much energy the body needs just to keep everything running.
Metabolism changes throughout the day based on activity level, food intake, age, muscle mass, and hormonal signals. A person with more muscle mass, for example, tends to burn more energy at rest.
Signs often associated with a slower metabolism include fatigue, easier weight gain, and feeling cold more often, while a faster metabolism may show up as increased hunger and difficulty maintaining weight.
Although many factors are beyond direct control, lifestyle habits like regular physical activity and balanced nutrition can support a healthier metabolic pattern.
3. Hormones Fluctuate More Often Than You Think
Hormones are chemical messengers that travel through the bloodstream to coordinate a wide range of body functions.
They influence mood, appetite, stress response, growth, reproduction, and sleep, often shifting subtly throughout the day. These fluctuations are tightly linked to both metabolism and circadian rhythms, creating a complex but coordinated internal communication system.
Cortisol, sometimes referred to as the body’s primary “stress hormone,” typically rises in the morning to promote alertness and gradually falls later in the day. Melatonin, by contrast, increases in the evening to help the body prepare for sleep. Insulin is released in response to food to regulate blood sugar, according to Cleveland Clinic.
When hormone levels become imbalanced, a person may notice symptoms such as mood swings, changes in weight, fatigue, irregular periods, or disrupted sleep. These shifts can be early clues that the body’s regulatory systems need attention.
4. Inflammation Happens Even Without Obvious Injury
Inflammation is often imagined as swelling or redness after an injury, but it is also a normal part of the immune system’s response inside the body. In the short term, inflammation helps fight infections and repair damaged tissue.
This type, known as acute inflammation, is usually helpful and temporary, appearing after events like a cut, a sprained ankle, or a viral illness.
Problems arise when inflammation becomes low-grade and long-lasting. Chronic inflammation can be driven by a variety of factors, including ongoing stress, smoking, highly processed diets, or lack of sleep and physical activity.
Over time, this persistent inflammatory state has been linked to conditions such as heart disease, type 2 diabetes, and certain autoimmune disorders.
While inflammation itself is a protective tool, noticing patterns like ongoing joint discomfort, digestive issues, or unexplained fatigue may be a reason to pay closer attention to lifestyle habits and medical checkups.
5. Circadian Rhythms Do More Than Control Sleep
Circadian rhythms are the body’s internal 24-hour clocks that synchronize many processes with day and night. These rhythms influence sleep-wake cycles, body temperature, hormone release, metabolism, and even immune function.
Light is one of the strongest signals for these internal clocks, especially natural morning light, which helps set the timing for alertness and energy during the day.
When circadian rhythms are consistently disrupted, through shift work, irregular sleep schedules, frequent late-night screen time, or crossing multiple time zones, health can be affected in subtle and not-so-subtle ways.
People may notice poor sleep quality, daytime sleepiness, irritability, difficulty concentrating, or changes in appetite and weight, as per Harvard Health.
Over the long term, misaligned circadian rhythms can contribute to metabolic and cardiovascular issues. Supporting these rhythms by keeping regular sleep and wake times, getting daylight exposure, and limiting bright light late at night can help the body’s internal clock run more smoothly.
6. Micro-Adjustments That Keep the Body in Balance
Beyond these more noticeable systems, the body constantly makes tiny adjustments to maintain balance, a state known as homeostasis. It fine-tunes temperature by making a person sweat when overheated or shiver when cold.
It maintains hydration by triggering thirst and adjusting how much water the kidneys conserve. Blood pressure and heart rate are constantly regulated in response to posture, stress, and physical activity.
These micro-adjustments generally occur without any awareness but are crucial for survival.
When the underlying balance is disturbed, such as frequent dizziness when standing, chronic dehydration, or persistent exhaustion, it can indicate that the body is working harder than it should to keep systems stable.
Paying attention to these small but persistent changes can help people recognize when something deserves further evaluation.
How Everyday Body Signals Can Guide Better Health
Reflexes, metabolism, hormones, inflammation, and circadian rhythms form a tightly connected network that shapes how the body performs from moment to moment. A shift in sleep can alter circadian rhythms, which may change hormone patterns, influence metabolism, and even affect how the immune system and inflammation behave.
Instead of viewing these processes in isolation, it is helpful to see them as parts of one larger picture of health.
By noticing recurring signs, such as ongoing fatigue, changes in appetite, persistent pain, difficulty sleeping, or heightened sensitivity to stress, individuals can gain a clearer understanding of what their bodies may be signaling.
While only a healthcare professional can diagnose underlying conditions, paying attention to these everyday processes can prompt timely conversations and proactive choices.
Recognizing how reflexes, metabolism, hormones, inflammation, and circadian rhythms behave from day to day turns the body’s automatic functions into a useful guide for protecting and improving long-term health.
Frequently Asked Questions
1. Can someone improve their reflexes with practice?
Yes. While basic reflex pathways are automatic, activities like balance training, sports drills, and reaction-time exercises can help the brain and muscles respond more efficiently.
2. Does eating at irregular times affect metabolism and circadian rhythms?
Yes. Frequently eating late at night or on an irregular schedule can disrupt circadian rhythms and may negatively influence metabolism and blood sugar regulation over time.
3. Can chronic stress change hormone levels and inflammation at the same time?
Yes. Ongoing stress can keep cortisol elevated, which may disturb other hormones and contribute to low-grade, chronic inflammation in the body.
4. How quickly do circadian rhythms adjust after changing sleep schedules or time zones?
On average, circadian rhythms may shift by about 1–2 hours per day, so full adjustment to a major schedule change or time zone can take several days.
All orders are protected by SSL encryption – the highest industry standard for online security from trusted vendors.
Happy Healing Girl is backed with a 60 Day No Questions Asked Money Back Guarantee. If within the first 60 days of receipt you are not satisfied with Wake Up Lean™, you can request a refund by sending an email to the address given inside the product and we will immediately refund your entire purchase price, with no questions asked.
We need the wisdom of cool heads and open hearts more than ever, and part of how we get to that wisdom is by (counterintuitively) allowing the fullness of our human experience, including our anger. Here we revisit a Q&A with Rhonda Magee as she explores the complexity, frustration, and intimate beauty of learning to make and be peace in the world.
Stephanie Domet: In your book The Inner Work of Racial Justice, you detail the steps you took to help one of your students process his attitudes and biases. What kind of energy does that work require?
Rhonda Magee: It requires a certain kind of commitment, a certain willingness to turn toward that which we could so easily deflect, turn away from, deny, minimize, avoid. For me it’s really important that when these opportunities present themselves for us to look into what’s arising around this, we turn in to that opportunity as opposed to away from it. I also think it takes a kind of grounding in a certain kind of love—kindness, loving-kindness— for me it takes some feeling of the value, of the possibility of connecting across lots of difference and the importance and value of trying to do it, again and again, even when it’s difficult.
SD: Why is it worth it to you to do this work?
RM: In my view, absolutely everything is connected, and that means all of us are connected, and so it seems to me that when we have these opportunities to expand the sense of our common ground, and we don’t take advantage of them and we don’t do what we can to heal and repair and transform the world, then it seems to me we are in effect contributing to barriers and obstacles to deep well-being. And so for me it’s worth it because it’s about practice. It arises out of deep practice for me—it arises out of the deep ethical ground of my practice.
SD: Who does that work serve? Is it for yourself, for the other person, the greater good of society? To honor the practice?
RM: It serves life. The gift of literally being alive. To me that’s not about any one of us, actually. To be alive is a great gift, and therefore the only real response to such a gift is gratitude. And a way to show gratitude is to try to minimize harm wherever it arises, as best we can. Recognizing we’re not perfect, that we’re not always able to see clearly how what we’re doing contributes to harm, we’re all vulnerable and misguided in our own ways, so it’s with a lot of humility that I say this. But ultimately, I think this question of who does it benefit, it benefits life.
SD: For a racialized person, a racialized woman, there are microaggressions everywhere. How do you take care of yourself to ensure you can do this work you want to do and feel called to do?
RM: It has come out of a sense of my own agency and what I often call personal justice. This idea that justice starts with us, how we treat ourselves. Taking care of myself feels like the first approximation of whatever it is I’m trying to offer in the world. There’s a reason I live in San Francisco as opposed to North Carolina or Virginia, where I was born and raised. The environment in San Francisco seems a bit more conducive to this way of accepting people, working across cultures, multiculturally, working with people who have different ways of expressing themselves, whether it be about race, sexual orientation, religion, immigration status. I specifically talk about the environment first and then the practices. We tend to think that from the practices we can overcome just about everything and that’s a good way to think, but I don’t want to miss this opportunity to name the relevance of our embeddedness in the world, and what’s possible is, in some measure, aided and abetted and shaped by the circumstances, the environments, the structures and systems that we find ourselves bathing in all the time. I live in a community that provides a certain amount of buffer against some of the worst kinds of disrespect that a person like me might find out in the world. From this place of relative protectedness, then I actually am able to give even more. We have to keep fighting for opportunities for people who today are suffering from a new set of oppressive systems.
SD: I wonder about your take on callout culture, or cancel culture. Is there a value in that approach, too? Your approach is one on one, which feels righteous, but slow. But what about other big-impact approaches? Do they also move the ball down the field?
RM: In the social justice arenas we may have overamplified some of the sharper ways of dealing with this. That’s not to say there aren’t times when we really need to take a strong, sharp stand. It takes a certain skill to act firmly and clearly and do so in a way that can minimize rather than exacerbate patterns of disconnect and separation. For me it’s never about just changing places with the people or processes that have been causing harm. It’s really about bringing around a new way of being with each other. There’s a certain urgency to figuring out how to work for some notion of justice and how to end oppression, but how to do that in a way that opens the heart, and that expands the capacity of all of us to be agents of a kind of public love that can help us sustain human life. Because the universe is going to go on in whatever way, but human life is vulnerable right now because of our failure to figure out how to live more gently and effectively together on this planet and to appreciate this brief opportunity we have between the birth and the death date to make a positive impact on this world.
“There is a way that even in the darkest times—intergenerationally dark times where there’s no reason to think your children will ever get out of this—there’s a way to love.”
SD: Do you ever lose your cool?
RM: I often lose my cool intentionally, as a tool for my own healing. If I’m feeling agitation and despair or some sudden rage at something I hear that seems completely nuts, my own practice journey at the moment is allowing those feelings to be expressed and as much as possible doing that regularly enough that they’re not creating a boiler that is going to explode out there. So if I’m here, at home, where it’s safe, it’s part of my practice to let the anger and the rage that I feel about injustice come right out. There are so many things happening that if you are willing to look at these difficult issues—I mean, my heart is breaking all day every day. I hum, I sing more nowadays, I hum and sing with others more nowadays. Singing, holding hands, humming, those are ways that human beings have across times and cultures managed to get through difficult times together. I sometimes forget just how many generations of human beings before recorded human history—for hundreds of thousands of years we don’t know the numbers of battles, rages, the despair, the inhumanity to each other, and yet we survived, and yet we didn’t burn down the planet, and yet we figured out how to keep getting up every day and feeding the children. There’s a planet’s worth of wisdom about how to get through difficult times and about the holistic nature of what that takes, so that’s what I’m about these days.
SD: I thought losing your cool would look more like—I don’t know—do you ever want to swipe all those books off the bookcase behind you?
RM: I mean, sometimes! When I hear this I’m tempted to think of those who say: We just need to start all over again. Blow it up and start all over. I don’t have kids, I’m not physically a mother, but I kind of feel like most moms and most of us in these communities that have suffered a lot over time, you know, we’re here. We’re usually not the ones who say let’s burn it all down. Because our children are in that. The things we have lovingly protected from the worst, as best we could through generations, whether through slavery or whatever our cultures and heritages have suffered through, we suffered through so we could live another day and find the sources of hope and regeneration. That mothering instinct, I believe it’s in all of us on some level, that instinct that would protect, that would go into the fire and pull out what we can and start again, mindfulness of that, cultivation of that is what I feel called to help support and that comes at least in part from my own particular lineage as the granddaughter of the granddaughter of formerly enslaved people. There is a way that even in the darkest times, intergenerationally dark times where there’s no reason to think your children will ever get out of this, there’s a way to love, to help bring about places where joy and healing can happen, and my goodness, if people could do it during much darker times, the holocausts of our history, the enslavement periods of our history—if it could be done then, then we can do it now. I have some love and compassion for those who feel so beleaguered that the call is just to burn it down. And I say, before you light that match, look into the eyes of a child, hold the hand of a friend, realize that these very human gestures matter, and look for that will, that capacity to live another day in love.
SD: When I look at what’s happening in the world today, the level of unrest and aggression, hate and burning, I see a lot of “men in the room.” What do you think about the role of women in helping bring about this “new way of being with each other”?
RM: I sometimes think of this in the conventional terms of identity—it seems obvious that we need more women in power! But I also think that more fundamentally and importantly, we need to see more empowered feminine energy in the world: that energy which lives in all of us—to greater or lesser degrees—the energy that nurtures, that cares, that sees the imprint of the future and the past in everyone and in everything we do. Any one of us can do this. And every one of us should.
https://vimeo.com/350988714 Whether we’re a teacher, whether we’re a director, whether we’re an administrative assistant, whatever we are because who we are and what our upbringing has been and what our life experiences have been is intricately a part of our authentic being. Unless we have taken time to look at… Read More
There’s a balancing of gender power happening across the professional world—including the mindfulness world. Twelve leaders in the field share how they claim their power and bring the diversity of their experiences in the mindfulness movement to bear in their work. Read More
Stephanie Domet is the author of two novels and a nonfiction book for middle grade readers. She’s the cofounder of the AfterWords Literary Festival and a contributing editor for Mindful. She lives in Kjipuktuk/Halifax, where she is, indeed, grateful to be alive, in the best way.
Endometriosis Pain Relief is a major priority for people living with chronic pelvic discomfort, painful periods, pain during intercourse, and bowel-related symptoms. Common endometriosis symptoms may also include bloating, fatigue, heavy bleeding, irregular cycles, and worsening pain before menstruation. Because symptoms vary widely, treatment often combines medication, lifestyle support, and targeted therapies to improve daily comfort.
Many patients also worry about the fertility impact of endometriosis, since inflammation, scarring, and ovarian changes can affect conception. Some studies estimate infertility may affect a significant number of people with the condition. A balanced plan using pelvic pain treatment, symptom control, and fertility-focused care can help protect long-term reproductive health while improving quality of life.
Endometriosis Symptoms and Initial Pain Relief Strategies
Endometriosis can cause a wide range of symptoms that affect daily comfort, energy levels, and reproductive health. According to Endometriosis UK, pain relief strategies often include anti-inflammatory medication, heat therapy, exercise, and speaking with a healthcare professional for long-term symptom management. Recognizing symptoms early and using supportive treatments may help improve quality of life.
Pelvic and Lower Abdominal Pain: Common endometriosis symptoms include persistent lower abdominal pain, pelvic pressure, and severe menstrual cramps that may interfere with daily activities.
Pain During Daily Functions: Some patients experience pain during intercourse, painful bowel movements, or discomfort during urination, especially during their menstrual cycle.
Cycle-Related Flare-Ups: Symptoms often worsen before or during menstruation, although some people may feel pain throughout the entire month.
Digestive and Energy Changes: Fatigue, spotting, constipation, diarrhea, and nausea may also occur, which can sometimes delay diagnosis.
Over-the-Counter Pain Relief: For early Endometriosis Pain Relief, many patients begin with medications such as paracetamol or anti-inflammatory drugs.
NSAIDs Dysmenorrhea Support: Ibuprofen or naproxen may help reduce inflammation and ease prostaglandin-related menstrual cramps.
Heat Therapy Comfort: Heat packs can relax tense muscles and provide short-term relief during painful flare-ups.
TENS Machine Support: TENS machines may help reduce pain signals through gentle electrical stimulation and can be useful for some patients.
Pelvic Pain Treatment: Hormonal and Advanced Medical Options
When pain becomes persistent, doctors may recommend pelvic pain treatment through hormonal suppression. Combined oral contraceptive pills are commonly used to reduce ovulation and slow the growth of endometriosis-related tissue. Continuous dosing may also reduce monthly flare-ups and improve day-to-day function.
Progestin treatments are another option for Endometriosis Pain Relief. These may include pills, injections, implants, or hormonal IUDs that help thin tissue and reduce bleeding. In more severe cases, hormonal therapy GnRH agonists such as leuprolide may temporarily lower estrogen levels, which can shrink active lesions and decrease pain.
According to the Cleveland Clinic, treatment for chronic pelvic pain may include hormone therapy, nerve pain medication, physical therapy, and multidisciplinary pain management when symptoms are ongoing or complex.
Fertility Impact: Surgical Interventions and Long-Term Management
The fertility impact of endometriosis depends on age, ovarian reserve, lesion severity, and scar tissue formation. Inflammation may affect egg quality or implantation, while adhesions can interfere with fallopian tube movement. Many patients still conceive naturally, but some need targeted fertility care.
When medication is not enough, surgery may be considered. Laparoscopic excision surgery is often used to remove visible endometriosis lesions while preserving healthy surrounding tissue. Surgeons may also treat endometriomas, release adhesions, or improve pelvic anatomy to reduce pain and support fertility goals.
Based on a study conducted by the National Institutes of Health, laparoscopic treatment of endometriosis may improve pain outcomes and may help selected patients with infertility depending on disease stage and overall reproductive factors.
Pelvic Floor Physiotherapy for Ongoing Endometriosis Pain Relief
Persistent endometriosis pain can affect pelvic muscles, movement patterns, and everyday comfort over time. Pelvic floor physiotherapy is often used alongside other treatments to help reduce pain and improve body function.
Muscle Tightness and Weakness: Ongoing pain can cause pelvic muscles to tighten, weaken, or lose coordination, which may worsen discomfort and pressure.
Comprehensive Physiotherapy Assessment: A physiotherapist may evaluate posture, breathing habits, muscle tension, and movement patterns connected to chronic pelvic pain.
Relaxation Training: Treatment may include techniques that help release muscle tension and improve pelvic floor relaxation.
Guided Stretching and Mobility Work: Stretching exercises can improve flexibility, reduce stiffness, and support smoother movement.
Muscle Release Techniques: Internal or external therapy methods may be used to reduce trigger points and improve muscle balance.
Improved Daily Comfort: Many patients report reduced pain during intercourse, easier bowel movements, and less guarding after regular sessions.
Post-Surgical Recovery Support: Pelvic floor physiotherapy may also help restore movement and comfort after surgery.
Exercise as Added Support: Yoga, Pilates, walking, and mobility exercises may complement physiotherapy and support long-term recovery.
Better Pelvic Pain Treatment Results: When combined with medication or hormonal care, physical therapy often improves overall pelvic pain treatment outcomes.
Comprehensive Endometriosis Pain Relief and Fertility Preservation Strategies
Managing endometriosis often requires more than one solution. Endometriosis Pain Relief may involve NSAIDs, hormonal medication, surgery, physiotherapy, and fertility planning depending on symptoms and goals. What works best can change over time, so regular follow-up remains important.
Early attention to endometriosis symptoms, careful treatment adjustments, and support for reproductive health can improve quality of life. Whether the priority is pain control, preserving fertility, or both, a personalized plan gives patients more options and better long-term confidence.
Frequently Asked Questions
1. What are the most common endometriosis symptoms?
Common endometriosis symptoms include pelvic pain, severe menstrual cramps, pain during intercourse, and bowel discomfort. Some people also experience bloating, fatigue, and irregular bleeding. Symptoms often worsen before or during periods. Severity does not always match how advanced the disease is.
2. What is the best Endometriosis Pain Relief option?
The best Endometriosis Pain Relief plan depends on symptoms, age, fertility goals, and disease severity. Some patients improve with NSAIDs, hormonal pills, or physiotherapy. Others may need surgery or advanced pain management. A personalized plan usually works better than a single treatment.
3. Can endometriosis affect fertility?
Yes, the fertility impact of endometriosis can be significant for some patients. Inflammation, scar tissue, and ovarian cysts may interfere with conception. Many people with endometriosis still become pregnant naturally or with treatment. Early fertility planning can be helpful.
4. Is surgery always needed for endometriosis?
No, surgery is not always required. Many patients manage symptoms through medication, lifestyle changes, and pelvic pain treatment programs. Laparoscopic excision surgery is often considered when pain is severe, fertility is affected, or imaging suggests advanced disease. The decision should be based on individual needs and medical advice.
Bread is a staple food in many households, yet researchers continue to study how certain types may influence body weight. While calories remain important, some studies suggest that bread weight gain may also be linked to how refined carbohydrates affect blood sugar, hunger, and fat storage. This may explain why some people gain weight even when calorie intake appears unchanged.
The type of bread eaten, portion size, and overall diet pattern all matter. White bread and other refined options digest quickly, while whole grain versions often contain more fiber and nutrients. Understanding why bread causes weight gain can help people make smarter choices without cutting out bread entirely.
Bread Weight Gain: High Glycemic Index Metabolic Mechanisms
Many refined breads are considered high glycemic index foods, meaning they can raise blood sugar quickly after eating. Rapid digestion causes glucose to enter the bloodstream fast, which may trigger a stronger insulin response. Insulin helps move sugar into cells, but frequent spikes may also encourage fat storage when repeated often.
According to the British Journal of Nutrition, higher intake of white bread and refined grain products has been associated with increased risk of overweight and abdominal fat gain in some population studies. Researchers noted that refined grains may affect appetite control and long-term weight trends differently than whole grains.
This helps explain why bread causes weight gain for some people more than others. Bread made with refined flour often has less fiber, which means it may not keep people full for long. That can lead to snacking later in the day and higher total calorie intake over time.
Why Bread Causes Weight Gain: Insulin Resistance Development
When refined bread is eaten frequently in large portions, the body may need to release insulin more often. Over time, cells can become less responsive, a process linked to insulin resistance mechanisms. When this happens, the body may store more energy as fat while blood sugar control becomes harder.
Based on information from Harvard T.H. Chan School of Public Health, diets high in refined carbohydrates may increase risk factors tied to type 2 diabetes and weight gain, especially when fiber intake is low. Whole grains, in contrast, are associated with better metabolic health and improved blood sugar balance.
This does not mean bread alone causes insulin resistance. Overall eating patterns, inactivity, sleep quality, genetics, and stress also matter. However, replacing frequent refined bread intake with higher-fiber foods may support healthier metabolism.
Calories and Weight Gain: Satiety Signaling Bread Disruptions
Many people focus only on calories and weight gain, but hunger and fullness signals also affect body weight. Foods that digest quickly may satisfy hunger at first, then leave people hungry again soon after. This can lead to larger portions at the next meal or extra snacks.
According to Healthline, white bread is often lower in fiber and digests faster than whole grain bread, which may reduce fullness and increase the chance of overeating. Fiber slows digestion, helps stabilize blood sugar, and can improve satiety after meals.
Refined carbohydrate metabolism may also play a role. Fast-digesting starches can create a quick rise and fall in blood sugar, sometimes followed by cravings. Choosing breads with seeds, whole grains, and higher fiber may help reduce this cycle.
Better Bread Choices to Reduce Bread Weight Gain
Choosing the right type of bread can make a difference when managing bread weight gain and improving overall nutrition. Small changes in bread selection may help control hunger, blood sugar, and daily calorie intake.
Choose Whole Grain Bread: Look for bread made with whole wheat, oats, rye, or other intact grains for more fiber and nutrients.
Check the Fiber Content: Pick options with at least 3 grams of fiber per slice to support fullness and digestion.
Limit Added Sugars: Some packaged breads contain extra sugar that may increase unnecessary calorie intake.
Watch Portion Sizes: Two slices may fit many meals, but oversized servings can add calories quickly.
Pair Bread With Protein: Add eggs, tuna, chicken, peanut butter, or Greek yogurt to help improve satiety.
Avoid Highly Processed Options: Ultra-soft refined breads often digest faster and may not keep you full long.
Read Ingredient Labels: Choose products with simple ingredients and whole grains listed first.
Rotate Carb Sources: Alternate bread with oats, brown rice, quinoa, or sweet potatoes for variety.
Smart Ways to Enjoy Bread Without Weight Gain
Bread does not need to be eliminated for healthy weight management. Portion size, bread type, and meal balance often matter more than bread itself. Choosing whole grain bread, pairing it with protein, and avoiding oversized portions can make a meaningful difference.
If you are concerned about bread weight gain, look at your total eating pattern rather than one food alone. Replacing refined options with higher-fiber choices, staying active, and managing overall calorie intake can support long-term health while still allowing bread in moderation.
Frequently Asked Questions
1. Does bread automatically cause weight gain?
No, bread does not automatically lead to weight gain. Weight changes usually depend on total calorie intake, food quality, and lifestyle habits. Some breads are more filling and nutritious than others. Portion size also matters.
2. Why does white bread make me hungry quickly?
White bread is often lower in fiber and digests faster than whole grain bread. This can cause blood sugar to rise and fall more quickly. Some people feel hungry again sooner after eating it. Pairing bread with protein or healthy fats may help.
3. Is whole grain bread better for weight control?
Whole grain bread often contains more fiber, vitamins, and minerals. Fiber can improve fullness and slow digestion. That may help with appetite control and steadier energy levels. It can be a better option for many people.
4. Should I stop eating bread to lose weight?
You do not always need to remove bread completely. Many people lose weight while still eating moderate portions of quality bread. Focus on overall diet balance and activity levels. Sustainable habits usually work better than strict elimination.
All orders are protected by SSL encryption – the highest industry standard for online security from trusted vendors.
Booster Brew | Sales Page | CB-R-1 | Cloned at: 2026-02-12 08:36:01 – Get Booster Brew is backed with a 60 Day No Questions Asked Money Back Guarantee. If within the first 60 days of receipt you are not satisfied with Wake Up Lean™, you can request a refund by sending an email to the address given inside the product and we will immediately refund your entire purchase price, with no questions asked.