What are the pros and cons of relative risk, absolute risk, number needed to treat, and average postponement of death when taking cholesterol-lowering statin drugs?
In response to the charge that describing the benefits of statin drugs only in terms of relative risk reduction is a “statistical deception” created to give the appearance that statins are more effective than they really are, it was pointed out that describing things in terms of absolute risk reduction or number needed to treat can depend on the duration of the study.
For example, let’s say a disease has a 2% chance of killing you every year, but some drug cuts that risk by 50%. That sounds amazing, until you realize that, at the end of a year, your risk will only have fallen from 2% to 1%, so the absolute reduction of risk is only 1%. If a hundred people were treated with the drug, instead of two people dying, one person would die, so a hundred people would have to be treated to save one life, as shown below and at 1:01 in my video How Much Longer Do You Live on Statins?.

But there’s about a 99% chance that taking the drug all year would have no effect either way. So, to say the drug cuts the risk of dying by 50% seems like an overstatement. But think about it: Benefits accrue over time. If there’s a 2% chance of dying every year, year after year, after a few decades, the majority of those who refused the drug would be dead, whereas the majority who took the drug would be alive. So, yes, perhaps during the first year on the drug, there was only about a 1% chance it would be life-saving, but, eventually, you could end up with a decent chance the drug would save your life after all.
“This is actually the very reason why the usage of relative risk makes sense…” Absolute risk changes depending on the time frame being discussed, but with relative risk, you know that whatever risk you have, you can cut it in half by taking the drug. On average, statins only cut the risk of a cardiovascular “event” by 25%, but since cardiovascular disease is the number one killer of men and women, if you’re unwilling to change your diet, that’s a powerful argument in favor of taking these kinds of drugs. You can see the same kind of dependency on trial duration, looking at the “postponement of death” by taking a statin. How much longer might you live if you take statins?
The average postponement of death has some advantages over other statistics because it may offer “a better intuitive understanding among lay persons,” whereas a stat like a number needed to treat has more of a win-or-lose “lottery-like” quality. So, when a statin drug prevents, say, one heart attack out of a hundred people treated over five years, it’s not as though the other 99 completely lost out. Their cholesterol also dropped, and their heart disease progression presumably slowed down, too, just not enough to catch a heart attack within that narrow time frame.
So, what’s the effect of statins on average survival? According to an early estimate, if you put all the randomized trials together, the average postponement of death was calculated at maybe three or four days. Three or four days? Who would take a drug every day for years just to live a few more days? Well, let’s try to put that into context. Three or four days is comparable to the gains in life expectancy from other medical interventions. For example, it’s nearly identical to what you’d get from “highly effective childhood vaccines.” Because vaccines have been so effective in wiping out infectious diseases, these days, they only add an average of three extra days to a child’s life. But, of course, “those whose deaths are averted gain virtually their whole lifetimes.” That’s why we vaccinate. It just seems like such a small average benefit because it gets distributed over the many millions of kids who get the vaccine. Is that the same with statins?
An updated estimate was published in 2019, which explained that the prior estimate of three or four days was plagued by “important weaknesses,” and the actual average postponement of death was actually ten days. Headline writers went giddy from these data, but what they didn’t understand was that this was only for the duration of the trial. So, if your life expectancy is only five years, then, yes, statins may increase your lifespan by only ten days, but statins are meant to be taken a lot longer than five years. What you want to know is how much longer you might get to live if you stick with the drugs your whole life.
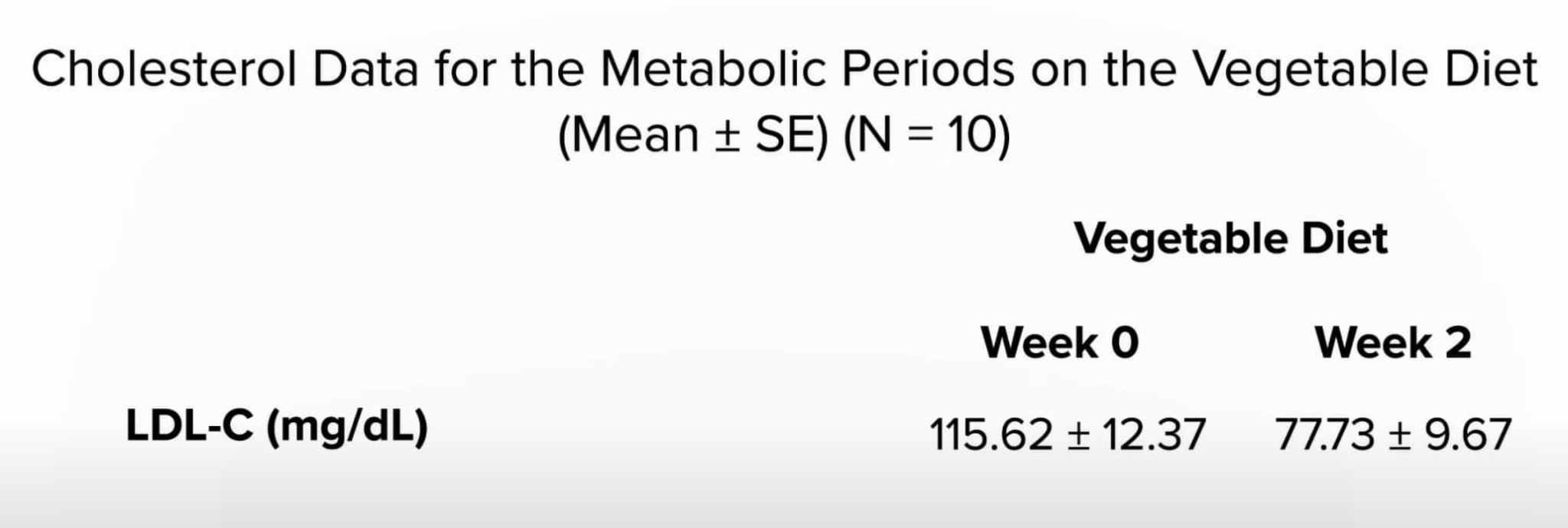
In that case, it isn’t an extra ten days, but living up to ten extra years. Taking statins can enable you to live years longer. That’s because, for every millimole per liter you lower your bad LDL cholesterol, you may live three years longer and maybe even six more years, depending on which study you’re reading. A millimole in U.S. units is 39 points. Drop your LDL cholesterol by about 39 points, and you could live years longer. Exercise your whole life, and you may only increase your lifespan by six months, and stopping smoking may net you nine months. But if you drop your LDL cholesterol by about 39 points, you could live years longer. You can accomplish that by taking drugs, or you can achieve that within just two weeks of eating a diet packed with fruits, vegetables, and nuts, as seen here and at 5:30 in my video.

Want to know what’s better than drugs? “Something important and fundamental has been lost in the controversy around this broad expansion of statin therapy.…It is imperative that physicians (and drug labels) inform patients that not only their lipid [cholesterol] levels but also their cardiovascular risk can be reduced substantially by adoption of a plant-based dietary pattern, and without drugs. Dietary modifications for cardiovascular risk reduction, including plant-based diets, have been shown to improve not only lipid status, but also obesity, hypertension, systemic inflammation, insulin sensitivity, oxidative stress, endothelial function, thrombosis, and cardiovascular event risk…The importance of this [plant-based] approach is magnified when one considers that, in contrast to statins, the ‘side effects’ of plant-based diets—weight loss, more energy, and improved quality of life—are beneficial.”