
Billion-dollar drugs have been pulled from the market for less carcinogenic contamination than is found in a single serving of grilled chicken.
In 2018, one of the bestselling blood pressure drugs, valsartan—sold as Diovan—was found to be contaminated by the “probably carcinogenic” nitrosamine known as N-nitrosodimethylamine (NDMA). It’s believed that about 20 million people worldwide were prescribed the drug tainted with this contaminant, which has a cancer risk shown to exceed that of many known potent carcinogens, such as asbestos, PCBs, and benzo[a]pyrene.
As I discuss in my video Cancer-Causing NDMA in Medications (Zantac, Metformin) and Meat, the U.S. Food and Drug Administration (FDA) estimated that taking the drug for a few years could cause cancer in as many as 1 in 8,000 people, whereas the European equivalent of the FDA estimated the cancer risk could be as high as 1 in 5,000. It is unlikely, researchers wrote in this 2019 paper, that drugs like valsartan are “a unique case.” And indeed, a few months later, the FDA announced it had found NDMA in ranitidine. Ranitidine, the acid reflux drug sold as Zantac, is one of the most prescribed drugs on the planet, in addition to being sold over the counter.
Then in 2020, some formulations of metformin, a popular diabetes drug sold as Glucophage, were found to be contaminated. The finding of NDMA in common medicines led the FDA to call for the immediate withdrawal of all Zantac from store shelves, yanking the drug from the market because its testing showed NDMA levels could, in some circumstances, exceed the acceptable daily intake limit of 96 nanograms per day. It was so bad that the FDA found levels of this carcinogenic contaminant in Zantac are similar to the exposure levels you would experience if you ate grilled or smoked meats!
Wait, what?
NDMA has not only been found in contaminated drugs. It is a known byproduct of tire plants, pesticide manufacturing, and leather tanning, and it is found in food and beverages, including processed meat and beer. Now that we know NDMA can transfer through the placenta, this may explain the relationship between maternal cured meat consumption during pregnancy and the risk of childhood brain tumors. For example, eating hot dogs while pregnant may increase childhood brain tumor risk by 33%, and sausages by 44%. Bacon consumption may increase childhood brain tumor odds by 60 or 70%. But it’s not just processed meat. Researchers have found it in poultry products as well. A single serving of chicken contains more than 100 nanograms of NDMA, as you can see below and at 3:02 in my video.
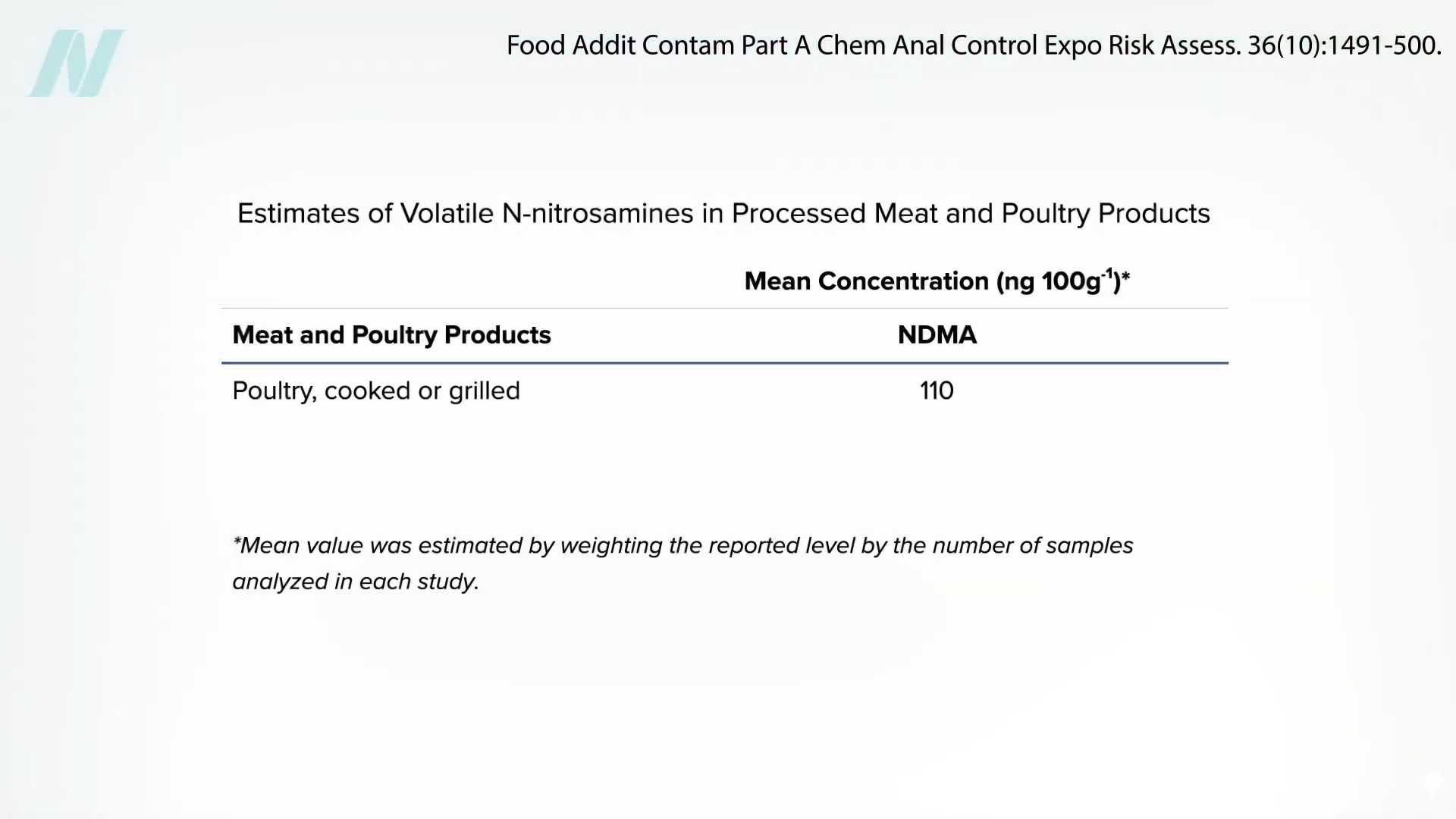
Remember how the FDA said the acceptable daily intake limit is 96 nanograms? Just half a chicken breast contains 110 nanograms.
Now, raw poultry doesn’t have any NDMA; it comes from the cooking process. In fact, the dry-heat cooking of meat, like broiling or grilling, even creates airborne NDMA, releasing this very potent carcinogenic compound into the air. So, even if you’re getting a salad at a charcoal grill restaurant, just being indoors where meat is being grilled could be a significant cancer risk.
Nitrosamines are also found in cigarette smoke, and pressure was put on the tobacco industry to try to remove them, arguing “there is simply no logical reason why a removable carcinogen should be allowed to remain in a consumer product….” That’s the same reason Zantac was yanked from store shelves.
Okay, so let’s get this straight. Zantac—which is one of the best-selling drugs in history, bringing in billions of dollars—was pulled from the market because it contained a probable carcinogen that exceeded the acceptable daily limit, but there may be more of the contaminant in a single serving of chicken?! So, my question is: Why aren’t they pulling poultry off the shelves, too?
Doctor’s Note
NDMA is a nitrosamine, a class of carcinogens also found in processed meat. See, for example, How Much Cancer Does Lunch Meat Cause?.
How can you make meat less cancer-causing? See Carcinogens in Meat.
Is Organic Meat Less Carcinogenic? Check out the video to find out.
Note: The article shown at minute 1:04 of the video I reference has since been retracted due to analytical artifact.


